

Part III in a four part series on health outcomes affecting Black Minnesotans. You can read Part I, about breast cancer disparities, here. Part II on sickle cell disease here.
Zhara Danelle Dooley grew up in the Rondo neighborhood of St. Paul, very close to Interstate-94. For as long as she can remember, she’s had asthma.
“I grew up next to a highway,” she said. “You never really think about it just because it’s part of life. It’s (Interstate) 94. It’s not a big deal. But then, when you think about how bad the air quality can be. That’s a big thing.”
While being in the top 50% for lung health in the nation, Black Minnesotans face stark health disparities compared to white people living in the same state. When it comes to lung health in Minnesota, there’s a line connecting it to air pollution exposure.
In the Twin Cities, the highest estimated rates of air pollution-related death and disease are found in neighborhoods with the largest percentage of Black, indigenous and people of color (BIPOC), low-income and uninsured residents and people who live with a disability.
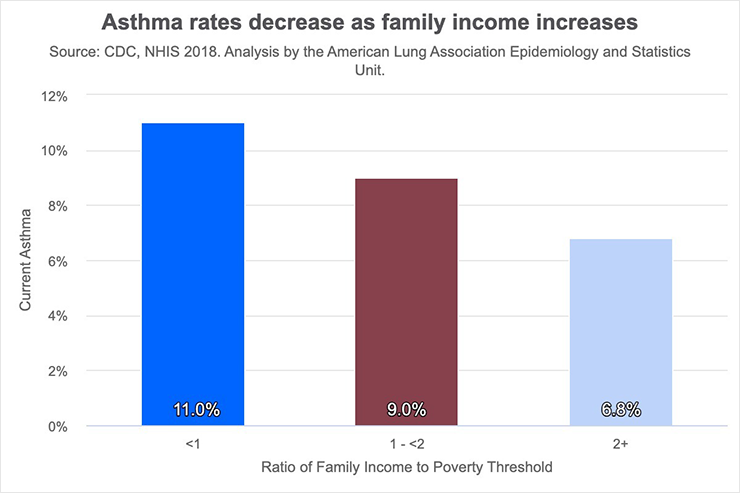
Nationally, that is also true. Black people are 42% more likely than whites to have asthma and have a mortality rate from asthma 2.8 times that of white people, according to data from the American Lung Association.

“In Minnesota, overall, we have relatively good health outcomes, but of course, some varying disparities in a variety of areas for people of certain races and other groups,” said Dr. Abbie Begnaud, an associate professor at the University of Minnesota Medical School and a physician at M Health Fairview. “With regard to lung health, a lot of the racial differences that we see are related to – almost certainly systemic inequities – probably in terms of environmental exposures.”
Zip codes with the largest percentage of BIPOC residents had more than five times the rate of asthma emergency room visits related to air pollution compared to areas with more white residents, according to the 2022 Life and Breath report by the Minnesota Department of Health (MDH) and Minnesota Pollution Control Agency (MPCA).
“That’s pretty stark evidence of disparities and who’s bearing the brunt of air pollution,” said Stephanie Fitzgerald, an attorney with the Minnesota Center for Environmental Advocacy.
State Sen. Bobby Joe Champion (DFL-Minneapolis) views pollution as a threat to health and wealth.
“Whether it’s an incinerator, brownfield, landfill, pollutants in the air from commercial areas, traffic congestion … are usually placed in our communities of color,” said Champion.
Historically, people of color have been subjected environmentally poor living conditions. For example, in St. Louis, Missouri, in the 1950s and ‘60s, as part of a military experiment, certain neighborhoods – which were predominately Black – were regularly sprayed with a mist that was later revealed to be zinc cadmium sulfide, a toxic substance.
Living with asthma
Asthma affects people’s day-to-day and often many of the choices they make. Dooley, for example, is very cautious about poor air quality and making sure she doesn’t worsen her asthma.
Her asthma attacks would sometimes put her in the hospital, she said.
“The only way I can describe it is if you’re if you’re in a pool, and the water is up to your neck and you’re trying to breathe, but there’s pressure on your neck,” she said.
She keeps her inhaler handy, but that wasn’t financially possible until insurance began covering it in 2018 with her new job. At one point, it cost $40 out of pocket with insurance. But that’s not always affordable, she said.
“Even if you have a full-time job, you might just not have the money to pay for it,” Dooley said. “There are plenty of times where you get sent home from the hospital and they will give you a bunch of prescriptions and you have to figure out, ‘which ones can I afford?’ And although I need the inhaler, the prednisone might be more affordable at the time.”
Because of that financial barrier, there have been times when she hasn’t had an inhaler.
“Not having one, it’s like if a plane didn’t have emergency exits, and the plane crashes and no one can get out. For me, that’s my safety exit,” she said. “If I can’t breathe, at least I know that little puff of albuterol could save my life.”
During the pandemic, Dooley was always worried about what an asthma attack might cause.
Back in February 2020, before COVID was widespread in the U.S., she went to urgent care with symptoms like shortness of breath and low oxygen saturation levels.
“It was dipping; it just kept getting lower and I couldn’t breathe, and they kept sending me home,” she said. “One night I get home, and I’m just like, ‘If I don’t wake up in the morning, there’s nothing I can do about it. It was a scary time for me because I didn’t know what would happen if I got COVID.”
Biases in the health care system and from providers often minimize the pain Black patients are facing and lessen the quality of care, Dooley said.
“I went to urgent care several times, and they basically told me, ‘You’re fine.’ They thought I was over-exaggerating what I was going through. Being Black, a lot of times, you don’t get listened to when you go to the doctor. It’s really disheartening when you go to seek help and you can’t get it,” Dooley said. “One of my biggest fears is that there’s gonna be a day where I’m having an asthma attack, and I go to seek help, and I don’t get it and I die. That’s like one of my biggest fears.”
What can be done to reduce asthma rates?
Champion and other community advocates, like the Environmental Justice Table and COPAL (Comunidades Organizando el Poder y La Accion Latina), are pushing to pass a bill that would tighten the permitting allowances across the state. The bill would require regulatory agencies to look at all the factors in the suggested permit zone when the zone is located in an “environmental justice area of concern,” defined by census tracts where at least 40% of people reported income less than 200% of the federal poverty level, or at least 45% of the people identify as people of color or areas that are recognized as Indian country.
It also would require the permit requester to conduct an analysis of the cumulative impacts of its suggested expansion or alteration and mandates at least one public meeting before the requested permit is issued or denied.
Part of the cumulative impact is looking at how various permit requests will affect people of color. Champion and other advocates such as Fitzgerald see a need for more research into the impacts of factors like pollution are having on the health of people of color.
“The idea is to get something passed where decision makers, the PCA (Pollution Control Agency), have to look at environmental justice neighborhoods and say, ‘Is this community already overburdened with pollution?’ That has to be a serious factor in deciding whether or not to grant a permit,” said Fitzgerald, who is also an advocate of the bill.
Champion thinks state leaders need to advocate for these issues because the people that are directly impacted often can’t.
“(Pollution) is usually in poor communities, impacting the people who are usually not as politically savvy or they’re just trying to make it from day to day from paycheck to paycheck,” Champion said. “They don’t have time to even concentrate on what’s happening or advocate for themselves, and therefore their voice isn’t heard, and one is hearing or is aware of the challenges that they are experiencing.”
Minneapolis’ East Phillips neighborhood is one such neighborhood faced with an environmental challenge right now. Community members have been advocating for several months, trying to stop the city from expanding its public works location.
Advocates such as the East Phillips Neighborhood Institute say expansion would bring added pollution and exacerbate the existing lung health issues in the neighborhood. Asthma rates in that area are more than two times higher than the state average, according to the Minnesota Department of Health.
About 71% of East Phillips’ roughly 4,700 residents are people of color, and nearly one-third live below the poverty line, according to Minnesota Compass.
Dooley says reducing pollution by going carbon-free could help reduce asthma rates in communities. But she doesn’t see that happening any time soon.
“Those changes cost a lot of money. Who knows if they’re willing to spend the money to really invest in the health of the people,” she said. “If a lot of white kids were dying from asthma attacks, we’d hear more about it. Just like (how) Black and brown people were at the center of the crack epidemic, and no one did anything about it. But now we have opioids, which is a white centered thing, and now it’s like ‘We have to do something about it.’ Until it becomes a quote unquote white problem, nothing’s going to happen. They’re not gonna fix anything.”


The article does a good job about talking about people of color who live in poor neighborhoods.
It would be wonderful if Minneapolis and St, Paul and/or Hennepin and Ramsey county would do some cutting edge research to look at the experience of all racial ethnic groups who live in poor neighborhoods, including poor white people, African and other immigrants, homeless children, teens and adults, the LGBTQ community, those in institutional settings, those after release from prison and those with physical and mental disabilities.
Poverty makes much worse for everyone, but how heavily does is weigh on each of these groups? The Twin Cities had “diverse diversity” that probably rivals Hawaii, California and New York.
Data that lumps together Black people whose relatives came as slaves more than 200 years ago with first or second generation African refugees is misleading. Better data and more analysis would sort it out. Better research is an effective tool to counter conservatives who state unsupported opinions as facts.
Be curious to see how smoking rates correlate to these statistics.
Regarding the title of the article, is it because they are Black or because of where they live?
Did the businesses come after the neighborhoods were created or were the neighborhoods built around the businesses?
neighborhoods with the largest percentage of Black, indigenous and people of color (BIPOC), low-income and uninsured residents and people who live with a disability.
This is an overly broad designation, and is not on,y black people. In cities with a majority of people being in a ‘minority’ group, the distinction loses its validity.
It seems like occurrence of asthma is related to living in a city.
Too often using these descriptive statistics, or even correlations lead to a false assumption of a causal relationship.
One necessary comparison needed to prove this point is whether black people or BIPOC with the others included, who live in suburbs or rural areas have similar rates of asthma.